 You can read the revised article in the book:
You can read the revised article in the book: Introduction to Medical Equipment Repair The book also contains a chapter on preventive maintenance, with recommendations on how to perform the various tests. Click here for more information. |
Oxygen Concentrators |
by Frank Weithöner |
The oxygen concentrator produces oxygen by filtering the oxygen out of the ambient air.

The oxygen is delivered to the patient through a nasal cannula. The patient breathes surrounding air through the nose which is additionally enriched with the oxygen through the nasal cannula.
In Europe and the US oxygen concentrators are home care equipment. They are used by patients at home for long term oxygen therapy. In hospitals oxygen concentrators are not often found because the needed oxygen is provided there by the central gas supply or by oxygen cylinders.
In other regions, however, oxygen concentrators are very often found in hospitals of all levels. They are not only used in the wards but also in operating theatres and ICUs because a central gas supply usually does not exist and gas cylinders are too expensive and too difficult to obtain. In operating theatres the oxygen concentrator is connected directly to the anaesthesia machine.
Common oxygen concentrators are moveable on casters and weigh between 15 and 20 kg.

|
Patient with nasal cannula |
Oxygen
Oxygen is a colourless and odourless gas with the formula O2.The ambient air consists of 21% oxygen (O2) and 78% nitrogen (N2) but only the oxygen is vital for living beings. The oxygen is absorbed by the lungs and transported with the blood, which is pumped by the heart to all our body cells. The waste product of the cells is carbon dioxide (CO2) which again is transported with the blood and pumped through the heart back to the lungs where it is exhaled. If the human body does not get oxygen for more than a few minutes, unconsciousness and death result.
The hospital technician measures the oxygen concentration of an oxygen concentrator with an oxygen meter (oxygen analyser).
Medical doctors and nurses are interested in the amount of oxygen which is dissolved in blood of a patient. They measure the oxygen concentration of the blood with a pulse oximeter.
Dangers of oxygen
Highly concentrated oxygen promotes rapid combustion. The addition of concentrated oxygen to a fire increases its intensity greatly and can even support the combustion of materials which normally do not burn.For this reason it is not allowed to work with oil and grease on any material which comes in contact with oxygen. Oil and grease already burn under normal conditions and easily ignite together with oxygen.
|
Caution! Oxygen supports combustion. In high concentration almost everything will burn. All components and material which come in contact with oxygen have to be cleaned thoroughly. Do not go near to any open flames when using oxygen. The use of oil and grease is strictly forbidden. |
Oxygen concentrators in district hospitals
In smaller hospitals oxygen concentrators are often used as the main oxygen supply. They are used to replacing oxygen cylinders which are often too expensive or, specially in remote areas, not easy to obtain. This works well but there are some restrictions.The produced oxygen from a concentrator cannot be stored. Whenever oxygen is needed, the concentrator has to run. Therefore electricity must be available all the time. This is probably the biggest challenge, especially in remote areas where power fluctuations and long power outages are common. A simple power backup with a small UPS is not possible due to the high power consumption of an oxygen concentrator.
Also high air humidity causes problems in tropical countries and along the coasts. In such situations the granules in the sieve tanks clog rather fast and the concentrator becomes unusable.
Finally, lack of maintenance is a limiting factor. Oxygen concentrators are complex machines which need frequent maintenance by qualified technicians. In addition, special spare parts are needed.

Pros
 Oxygen is always available (when electricity is
Oxygen is always available (when electricity is present)
Produced oxygen is cheapCons
Electricity is always needed High power consumption (400 - 600 W) Battery back-up is not possible Frequent maintenance is needed Spare parts like filters for maintenance are needed
Special parts for repairs are needed Problematic in areas with high humidityConclusion: Oxygen concentrators are the better and cheaper option - as long as the electricity supply is assured or gas cylinders as a backup are available.
Usage
Before switching on the oxygen concentrator check the connected tubing for kinks and blockages. When the concentrator is used for therapy, fill the humidifier with the right amount of distilled water. The lid has to be closed firmly.Switch on the concentrator and wait at least for two minutes. Only then the oxygen concentration is high enough for usage. But even with low concentration in the beginning the machine delivers air so that you can check the tubing and the humidifier. If everything is all right, the humidifier makes bubbles.
All concentrators have a flow meter with an adjustment option for the flow rate, which is indicated by a little ball floating in a glass tube. Set the flow meter to the required flow value.
Finally check the alarm function. Pull the mains plug without switching off the concentrator. An alarm must sound.
Usage in areas of high humidity
The sieve filters are sensitive to humidity. When moisture enters the filters, the filter material swells up, clogs the filter and the oxygen cannot pass through any more. When this happens the filters have to be replaced then, which is often not economically. This is a big problem especially in coastal areas where the humidity of the air is very high. The only solution is simple: The concentrator has to run, even when it is not in use. When the concentrator runs the filters get flushed and thus also the humidity.This applies particularly to the concentrators in the storage rooms of the hospitals or to the ones of an equipment donation or other shipment which are left for late use in the container. Put them into operation as soon as possible or they are soon ready for the scrap heap!
|
Hint! A concentrator has to run regularly. Even when it is not in use, it
should be switched on for half an hour every week. |
Humidifier
Usually the oxygen concentrator is used for therapy and the oxygen is applied to the patient through a nasal cannula. To this end the oxygen has to be moistened, otherise the nasal mucosa of the patient would dry out.
In general the humidifier is connected directly to the outlet of the flow regulator without a tube in between. But sometimes the concentrator is not placed beside the patient but at a distance and a longer tube is needed. In this case it is better to add the long tube (≥ 2 m) between the concentrator and the humidifier. If a long tube would be connected after the humidifier, the moistened oxygen would condensate in the tube and the water would block the tube.

Another method to prevent condensed water in long tubing is to insert a 'water trap'. This is just a plastic tube with a bigger diameter where the condensed water gets collected. Therefore the 'water trap' has to be inserted at the lowest point and of course emptied frequently. For this reason it is always better to prevent condensation by moving the humidifier closer to the patient.
Filters
The user has access to two filters which have to be cleaned or changed frequently. First there is a coarse filter made out of foam. This filter absorbs the dust from the air at the air intake and should be cleaned once a week. The filter is washable. Directly after the dust filter follows another filter, a fine bacterial filter. This filter should be exchanged or at least checked twice a year. It is a disposable filter which cannot be cleaned.|
Caution! Never run the concentrator without a filter! |
Alarm
Concentrators are equipped with an audible alarm function. In case of a power outage or whatever the internal pressure gets too high or too low a beeper gives an alarm.Many concentrators also check the oxygen concentration at the outlet. When the concentration drops under approximately 80% the concentrator also gives a signal. During the first minutes when the concentrator does not yet deliver sufficient concentration, this alarm function is deactivated.
A 9 V back up battery provides the power for the alarm unit during times of power blackouts.
User manual
User manuals are always delivered with new oxygen concentrators. It is a good idea to copy the manual and leave one issue with the equipment and keep the other in a file with other technical manuals in the hospital workshop.With donated, used concentrators however the manuals are usually missing. In this case try to download the manual from the manufacturer's website. If this is not possible, try it under User manuals.
|
Tip! It is always a good idea to create a quick user chart with just a few
words in the local language about the usage and the cleaning. Such a quick user chart can be laminated in plastic and attached to the
concentrator or close to it to the wall. |
User maintenance
In order to keep the oxygen concentrator in good condition the user has to do regular checks and cleaning. The cleaning procedures should be integrated in the daily or weekly routine of the respective hospital department. Change the water of the humidifier daily and rinse the humidifier. Use distilled water only. Wash the intake air filter weekly. Let the concentrator run for half an hour every week if it is not in regular use.Common usage problems
The most common problems which occur during the usage are a blocked airway or a leaking humidifier.Here the typical problems and their causes:
No oxygen flow, no bubbles, ball not floating → Blocked tube, kinked
tube or water in the tube.
No oxygen flow, only a few bubbles, ball floating No oxygen flow, only a few bubbles, ball floating → Leaking humidifier, lid of humidifier not tight. Leaking humidifier, lid of
humidifier not tight.
The concentrator itself can also make trouble. In order to find out if the concentrator causes the problem or the attached accessories, disconnect everything from the concentrator. Close the outlet with your thumb. You should feel the pressure and the ball in the flow meter should fall (no flow).
Installation
Before an oxygen concentrator is purchased or set up some requirements have to be met. Is the power supply suitable, is the voltage correct? Does the machine have a suitable plug? Donated concentrators from the US (120 V) do NOT work in Africa on 230 V!
An additional transformer would be much too big and too expensive.
Is the electrical installation appropriate? The concentrator takes a lot of power (400 - 600 W).
Therefore you should not use cheap extension cables or cheap multi sockets.
The room should be dust free and well ventilated, not too hot and not too humid. The intake must be free and must not be covered at any time. Place the concentrator not too close to the wall, the patient bed or a curtain.
Avoid using long tubing, which creates problems with kinks and condensed water. Place the machine as close to the patient as possible.
When the concentrator is used in the operating room:
Place it away from other gases such as ether. Place an additional oxygen cylinder nearby with an easy change-over possibility in case of a malfunction or power outages.
Explain the correct usage to the user, the doctors and the nurses. Point out the problems with blocked and kinked tubes and explain the cleaning of the humidifier and the filter.
Finally hand over the user manual to the responsible person and let them sign a handover protocol. In such a form the user declares that the installation is completed, the machine is functioning and uses have been instructed.
|
Attention! It is NOT the task of the technician to give recommendations about the
application of oxygen in terms of flow rate or duration of treatment. |
Function
An oxygen concentrator uses molecular sieves (or sieve filters / sieve bed filters / sieve tank) that bind nitrogen and let oxygen pass through. Since this technology only works under high pressure, a compressor is needed. Behind the sieve filter the oxygen pressure is again reduced, the flow controlled and then delivered to the patient.Apparently the filters get saturated with nitrogen after a few seconds, so that the filters need to be flushed. This is done in reverse direction with a part of the just filtered oxygen. Therefore the inlet valve switches over to an exhaust opening. Because it takes time for building up pressure, flushing, switching over and releasing the nitrogen, the oxygen flow to the patient would be interrupted for some time. That is why oxygen concentrators always have two sieve filters which work alternately, one filters the oxygen while the other gets flushed. The slightly fluctuating oxygen pressure is then led into a buffer storage tank before it gets to the patient.
Here the functional process in detail:
Ambient air gets into the concentrator via a foam dust filter. One part of the air enters the compressor trough another fine filter, the other part is needed to cool the compressor unit. Behind the compressor a cooling coil with a fan cools down the warm compressed air before it gets into the sieve tank system.

1. Inlet valve V2 is open. Pressurized air from the compressor of 1.4-2 bar (20-30 psi)
enters sieve tank 1.
2. Oxygen passes through filter 1 but nitrogen accumulates at the filter intake.
3. The oxygen gets through a restrictor into the reservoir tank. Through another restrictor a
part of the oxygen enters sieve tank 2 through the outlet.
4. The trapped nitrogen of sieve tank 2 is flushed through the intake and gets through the
open exhaust valve V3 and the muffler out of the concentrator.
5. After 7-8 sec V1 and V3 close and the equalization valve V5 opens for 1 sec. The different
pressures of the sieve tanks get balanced.
6. Now V4 and V1 open. Air gets into sieve tank 2, oxygen from sieve tank 2 fills the
reservoir tank and sieve tank 1 gets flushed.
The reservoir tank is connected to a pressure regulator where the system pressure is reduced to patient pressure of 0.5 bar (8 psi). The flow can be adjusted with a flow meter within a range of 1 to 5 litres per minute. The value is shown by a little ball floating in a glass tube.
Between pressure reducer and flow meter another bacterial filter is inserted. This filter does not only protect the patient but also the concentrator of humidity from the outlet when the concentrator is not in use.
For safety reasons an internal measurement device for the oxygen concentration is often connected between the reservoir tank and the flow meter. When the oxygen concentration drops due to a fault, an alarm is given. The alarm will also sound when the system pressure is too high or too low.
Tools

A frequent check of the oxygen concentration is important, because a flow at the outlet (bubbles in the humidifier) does not necessarily mean that the concentrator produces oxygen. It can be just air or oxygen of low concentration. That is why the oxygen meter is the most important tool the hospital technician needs for the maintenance of concentrators. It is a must in every hospital workshop.
When the instrument is not used, the sensor should be stored in a sealed plastic box with a drying agent (silica gel) because it is sensitive to humidity.
The oxygen meter can be easily calibrated just by measuring the surrounding air. The display then should be set to 20.9%. Or attached to an oxygen cylinder it should display 100%. Breathing out from your lungs against the sensor, by the way, would let the concentration drop to approximately 17%.
Because the measurement of the oxygen concentration needs a certain flow the meter cannot be connected directly to the outlet but only via a T-piece. A piece of foam should then be inserted in the free outlet of the t-piece in order to simulate a little flow resistance.

Maintenance
An oxygen concentrator can easily reach 40,000 working hours or more - when it is regularly serviced.Cleaning
Humidifier, tubes and the inlet dust filter always have to be clean. It is the task of the user to clean them regularly. Nevertheless, the cleaning of the foam filter is also part of the maintenance. It can be washed with soap water but then it has to get dry before putting it back into place.The following bacterial filter is a single use bacterial filter. It should be replaced once a year or every 5.000 hours. I case of a doubt, take the filter out and check the segments. They have to be white and clean.
This also applies to the bacterial filter situated ahead of the flow regulator.
The outside of the concentrator should finally be cleaned with a mild soap solution.
Function check
After cleaning and replacing the filters make a function check, measure the oxygen concentration at different flow rates and test the alarm. Start with a visual check. Check the housing for damages. Check also the power cord, plug and wall socket.
Switch on the concentrator and let it run with humidifier and tubes. Bubbles must be created immediately and the little ball of the flow meter has to float freely.
Listen to the operating sound. Pumping and exhausting sounds of both cycles must sound identical. A complete cycle should have a period of 16-20 sec, depending on the
manufacturer.
Now block the outlet with your thumb. You should feel the pressure and the ball in the flow meter has to fall down. Listen to any hissing sound which indicates a leaking
system.
Disconnect the humidifier and connect an oxygen meter. The measurement equipment itself has to be calibrated before connecting to 21%. The concentrator should deliver full
concentration 2 - 5 minutes after switching on and the concentration should be between
90 and 95%.
Now check the flow. It should be adjustable between 1 and 5 l/min. The concentration may drop a bit when the flow is increased. But it should never be below 85% because
such a low oxygen concentration has no medical effect.
The alarm function and the alarm battery also have to be checked. Fore that the concentrator simply has to be disconnected from mains while it is running. The alarm
must sound.
Additionally check the 9 V alarm battery with a multimeter or replace it when it is older than two years.
Finally fill out the maintenance report. Do not forget to write down the actual working hours. It is very helpful when a problem occurs later. Many concentrators get problems
because they are NOT running (moisture in the sieve tanks). The hour counter will
indicate that.
Lubrication
Lubrication is not allowed on any material which comes in contact with oxygen. Oil and grease already burn under normal conditions and ignite together with oxygen.All connections which come in contact with oxygen have to be free from grease and oil. Even fingerprint have to be avoided. All connections should be wiped clean before assembling.
But there are special lubrication products on the market which are specially made for usage in combination with oxygen. Unfortunately they are difficult to obtain and furthermore
10-20 times more expensive than normal lubricants.
Possible products are:
Krytox GPL 205, 206, 224 Christo-Lube MCG 111 Klüberalfa YV 93-302 Zarox TYN142 Halocarbon 25-5SBut in principle do not lubricate and consult the service manual for recommendations.
Repair
As always, troubleshooting starts with observing and listening to the machine. Make a function check (see ↑Function check). Listen to any abnormal sound and check the switching times.If anything sounds abnormal, open the concentrator and have a closer look. Often the status of the valves are indicated by LEDs which are mounted on the control board.
Many concentrators also have ports where you can connect a pressure gauge. Consult the service manual. Here an overview about pressures and switching times:
Pressure compressor: 1.4 - 2.0 bar (20 - 30 psi) Pressure reservoir tank: 1.4 - 2.0 bar (20 - 30 psi) Pressure patient outlet: 0.5 bar (8 psi) Equalization time: 1 sec Half cycle (filtering or flushing): 7 - 8 sec Complete cycle: 15 - 18 secService manuals
While user manuals are relatively easy to obtain, service manuals are hard to come by. The manufacturers do not support the repair of their equipment by other technicians than their own.Service manuals for the most common concentrators you might under Service manuals.
Filters
A low oxygen concentration and a decreased gas flow can be the result of a blocked bacterial filter. Bacterial filters have a clear plastic housing and a dirty filter is easy to recognise. These are disposable filters which cannot be cleaned.If you do not have a spare filter, you have to wait with the repair until you have got the right one. Do not run the concentrator without it.
|
Tip! Different concentrators use different filter designs, but most of them have the
same connection system. If you have different concentrators in your hospital, it is worth to check the connection diameter. It may be that
you only have to provide one type and it will fit all your oxygen concentrators. |
|
Tip! Dust filters are simple foam filters and can be cut out of (mattress)
foam or better kitchen sponges. But be aware that you cut such filters thinner when the replacement foam is denser than the original. |
Sieve tanks
The sieve tanks are filled with zeolite granules, a synthetic aluminium silicate. Zeolite acts as a molecular sieve which binds the nitrogen molecules and lets the smaller oxygen molecules pass.Unfortunately zeolite also has the ability to absorb water which can cause problems in areas with high humidity.
Sieve tanks should last at least 20,000 hours, and when regularly maintained even 40,000 hours or more.
Typical problems
Sieve tanks tend to lose their filter properties over time. High humidity is often the reason. Water then condenses inside the filter and clogs the granules. Too high system pressure and low oxygen concentration is an indicator for a blocked filter. You will also get an asymmetric concentration measurement results because one sieve tank will deliver more oxygen than the others as the control circuit periodically switches between them.
A clogged sieve which contains water also weighs more. If it is 50 g heavier than a new one the sieve tank contains too much water and has to be exchanged.
Please note, that sieve tanks should always be replaced in pairs, even when only one is defect. In industrial countries this is not a problem, because the tanks can be ordered easily and the prices are reasonable. But in other countries the situation is different. Due to the high shipping costs it does not always make sense to repair the concentrator.

|
Tip! An oxygen concentrator has to run, at least half an hour every week. |
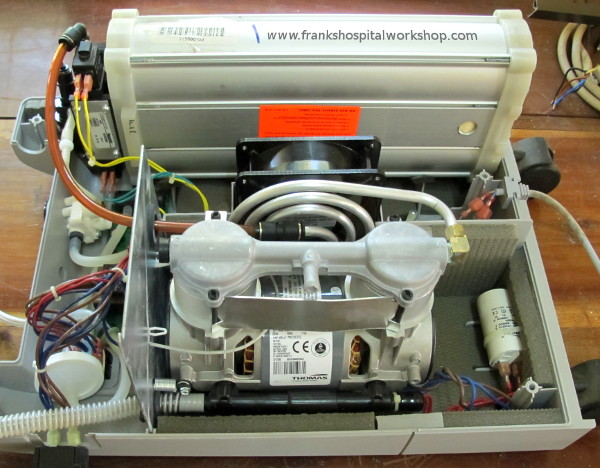
Compressor
The compressors in oxygen concentrators are piston type compressor with two pistons. A common type is the one from Rietschle Thomas. The working pressure is about 1.4 - 2.0 bar (20 - 30 psi).The compressor is driven by an asynchronous motor with a run capacitor.

Typical problems
A very common problem is a defective capacitor. In case the compressor does not start or blows the fuse or triggers the circuit breaker.
Keep also in mind that often a temperature fuse is often attached to the motor windings. It rarely blows without a reason, perhaps the pressure is too high and the motor got too
hot.
If the capacitor is OK and the motor is still not starting, maybe the compressor itself is stuck or the filters are blocked (resistance too big). Disconnect the hoses from the
compressor and restart the compressor.
When the head gasket leaks, it is usually audible. Leakages can be made visible by applying soup water with a brush to the suspect areas. The escaping air will then create
bubbles.
When the pressure is too low and no leakages recognisable, then the piston rings could be the problem. Consult he service manual for further instruction.
Control board
The control board generates the switching signals for the valves. In principle the electronics is simple and could be repaired easily but unfortunately the circuit diagram is never printed in the service manual.Anyway, it is worth to check the switching times. If they are wrong the concentrator will not create enough oxygen or worse, will not flush the humidity out of the filters which causes irreparable damage.
The times proximately are:
Filtering or flushing cycle: 7 - 8 sec Complete cycle: 16 - 20 sec Equalization time: 1 secValves / Valve block
For intake and exhaust two types of valves are found in oxygen concentrators. Either the valves for the sieve filters are controlled directly by solenoids or we find pneumatic valves which are controlled by a pilot air pressure also controlled by solenoids. The advantage of the latter solution is, that the solenoids only have to release the valves which does not need much force. For closing the valves the air pressure from the compressor is used.In total we find 5 valves, that is 2 intake valves, 2 exhaust valves and 1 equalization valve between the two filters. Intake valve 1 and exhaust valve 2 are always switched at the same time as well as intake valve 2 and exhaust valve 1.
Often the valves are not connected via tubes but they are embedded in a valve block which is directly mounted at the top of the sieve filters. Valve block and filters are then one mechanical unit.

For test purposes the block can be removed from the filters and be tested without them. You can then see the valve movements and feel the air pressure when closing the openings with your thumb.
Common problems
Sometimes the rubber diaphragms of the pneumatic valves tear. Then they have to be replaced.
Also the release pin of the solenoids tend to get stuck. A drop of WD-40 can often solve this problem.
|
Note! When disconnecting silicon tubes, do not pull the tube but push it
from the connector. When you pull, the tube diameter gets smaller and the connection tighter. |
Links and sources
Here are some Wikipedia Medical Equipment articles:Oxygen concentrator
Oxygen therapy
Oxygen mask
Oxygen
Nitrogen
Oxygen saturation
Oxygen sensor
|
You can read the revised article in the book: Introduction to Medical Equipment Repair The book also contains a chapter on preventive maintenance, with recommendations on how to perform the various tests. Click here for more information. |
 |
|